
Publicité
Out of the 20,000 expected COVID 19 cases only 324 has been detected
Par

Partager cet article
Out of the 20,000 expected COVID 19 cases only 324 has been detected

Introduction: Zero case of COVID-19 is a statistically improbable number from the daily moving average curve. This observation calls for caution in rushing to conclusions; prematurely declaring a peak is dangerous since absence of new cases may lead us to lower our guard and unintentionally spread the disease. We must a priori estimate the number of cases, monitor our surveillance and epidemiologically interpret the data before drawing any conclusions that may impact policy and programmatic actions.
Estimating the number of infected persons: Many scientists believe that SARS-COV-2 virus must infect between 60 to 80% of the population before the epidemic tails off. So, what is the actual number of Covid-19 cases in Mauritius now? We can intuitively estimate a bulk part figure based on the following empirical global assumptions: a) In a given population, one-third of infected persons are asymptomatic, b) two-third are symptomatic, c) 20% of symptomatic persons require medical intervention and are picked up by the surveillance system. So, if we back-calculate from the 324 reported cases, we will expect to have some 2,500 cases in the population, which has to be adjusted for the sensitivity of surveillance. If out of 2,500 expected cases, we are observing 324 cases, the sensitivity of our surveillance is around 13 percent (324/2,500). After adjusting for this sensitivity, we obtain a bulk part figure of approximately 20,000 cases comprising of symptomatic and asymptomatic persons. Where are those cases then? We are missing them because our surveillance is incomplete and we are not undertaking widescale testing.
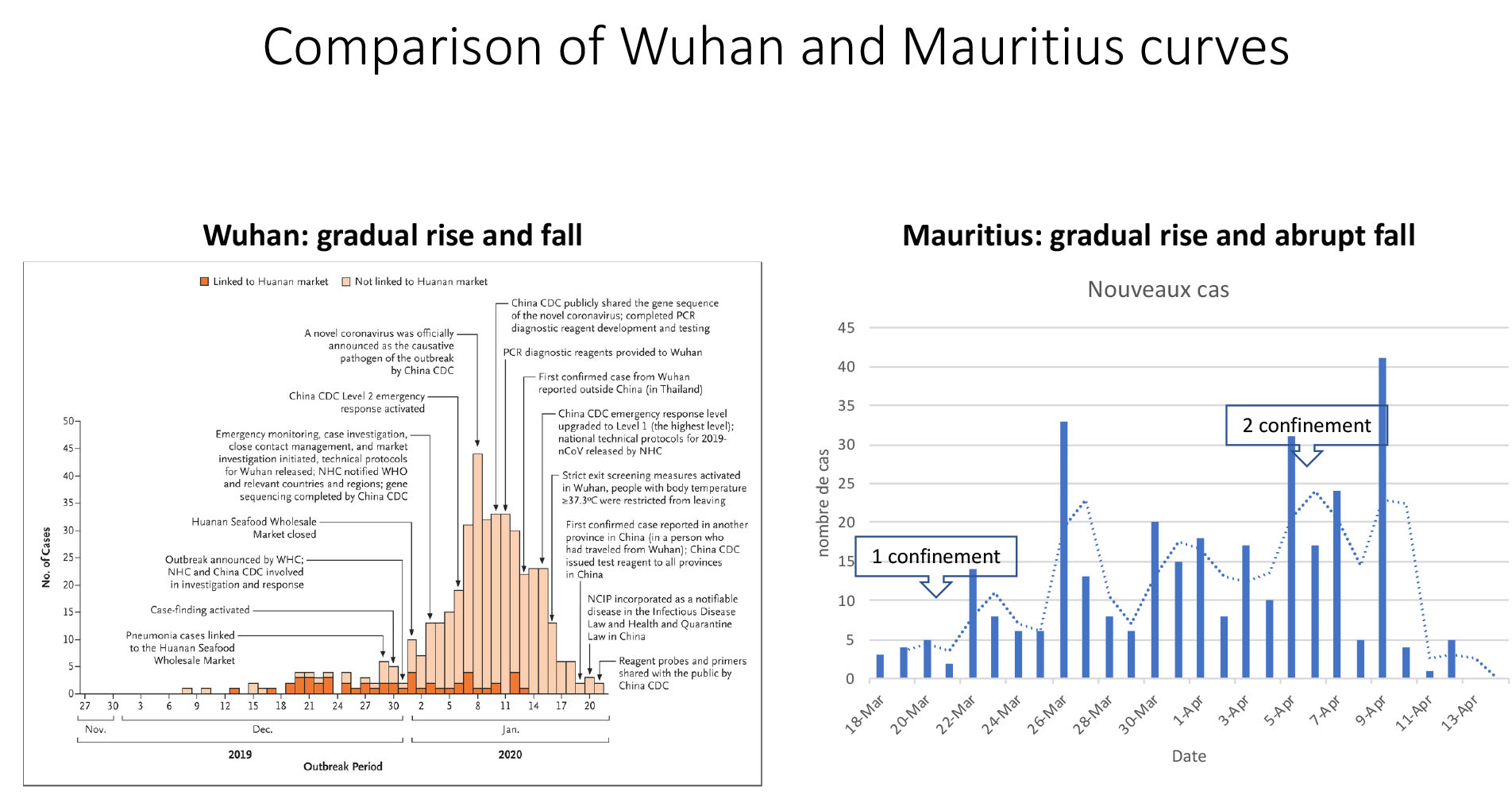
Epidemic curve: To get a visual display of the trend of daily cases, we use an epidemic curve to monitor how far we are from the goal post. The epidemic curve of Covid-19 in Wuhan pictorially shows that the curve rises and falls off symmetrically, as is typical of an infectious disease. By contrast in Mauritius, the curve rose smoothly but has asymmetrically dropped below the moving average. (See accompanying chart for illustration.) This asymmetric curve is impossible for an infectious disease that is transmitted from person-to-person: everybody is not synchronously infected and will therefore reach the endpoints at different times. Hence is it improbable to have zero case in such a narrow interval. The alternative and plausible explanation is the inability of the surveillance to find and test all cases.
Surveillance: Surveillance provides information for action when it is sensitive and complete: completeness means finding all the existing cases. Focussing on active case detection through contact tracing is only looking at the tip of the iceberg; it is a skewed convenience sample. What is needed is random sampling and widescale testing in flu clinics, front-line workers and persons residing in hot-spot areas. We have only detected 324 out of the 20,000 expected cases; we need to improve our surveillance.
Conclusion: The epidemic curve shows that our surveillance is incomplete and must be strengthened by random and widespread testing. Monitoring is imperative; if we prematurely call off a confinement we run the risk of second and more catastrophic wave, as seen in other countries.
Publicité
Publicité
Les plus récents




